Understanding and Treating Borderline Personality Disorder: A Shift from Disorder to Personality Style
Table of Contents
- Our BPD Therapists
- Understanding and Treating BPD
- DSM-5 Diagnostic Criteria for BPD
- What Does BPD Look Like in Everyday Life?
- How Does BPD Develop?
- Therapeutic Approaches to BPD
- How Can Deeper Emotional Healing be Achieved with BPD
- Psychotherapy and BPD
- Efficacy of ISTDP in Treating BPD
- Conclusion
- How to Book an Appointment for help with BPD
- FAQs About BPD
Borderline Personality Disorder: Symptoms, Causes and Treatments
Before we take an in-depth look at Borderline Personality Disorder (BPD), this section provides a concise overview, highlighting common symptoms, underlying causes, and effective therapeutic approaches.
Keep reading below for a comprehensive exploration into understanding and managing BPD.
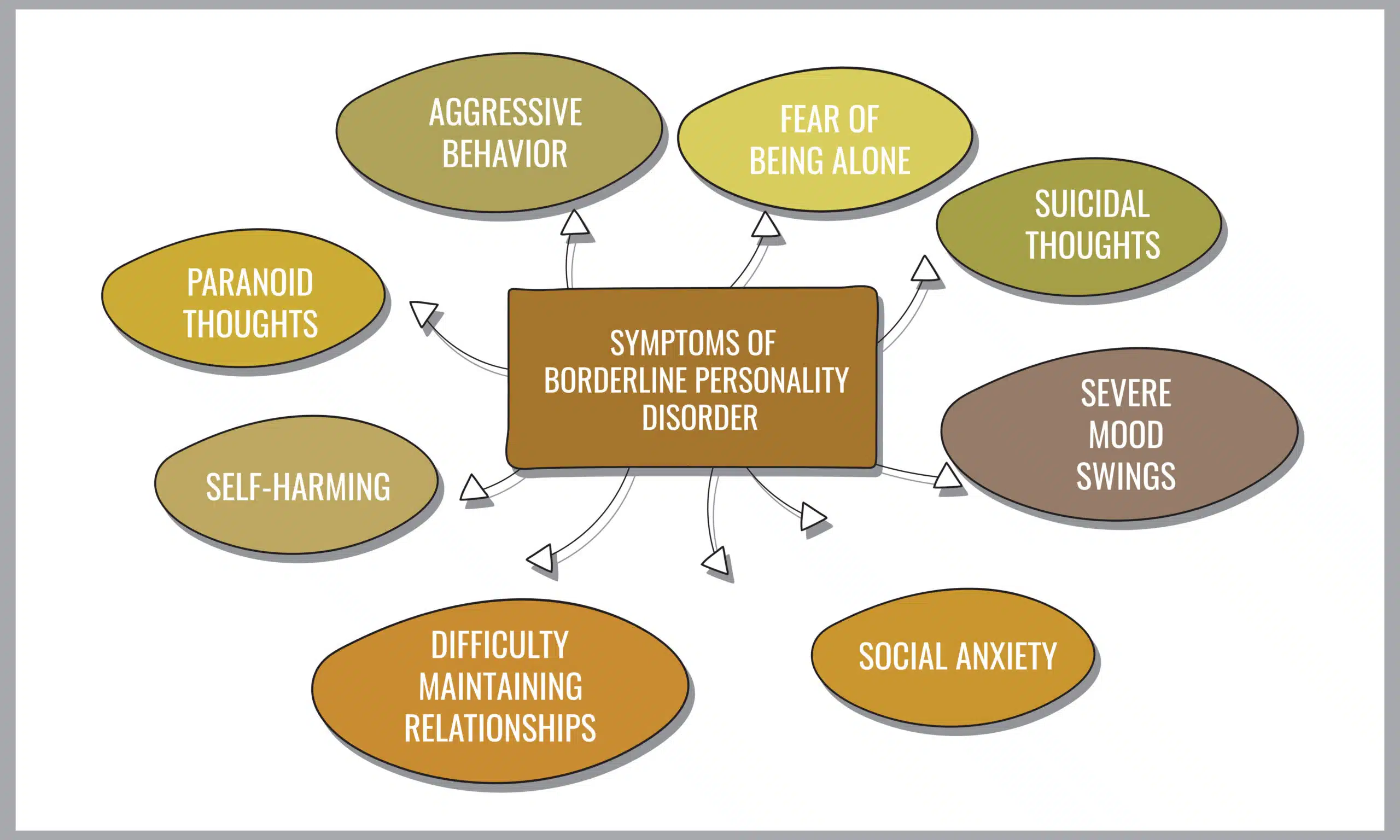
Common Symptoms of Borderline Personality Disorder
- Intense fear of abandonment, including efforts to avoid being left alone.
- Unstable and intense relationships, fluctuating between idealisation and devaluation.
- Unstable self-image or sense of self, often changing goals, values, and self-perception.
- Rapid mood changes, experiencing a range of emotions such as anger, anxiety, or sadness in a short span.
- Impulsive and potentially self-damaging behaviours, such as substance abuse or reckless driving.
- Recurrent self-harm or suicidal behaviour, often as a response to distress or perceived rejection.
- Persistent feelings of emptiness or boredom.
- Intense and inappropriate anger, difficulty controlling temper.
- Temporary paranoid thoughts or severe dissociative symptoms, often in response to stress.
Common Causes of Borderline Personality Disorder
- Experiences of abuse and trauma in childhood: Many people with BPD report histories of significant emotional, physical, or sexual abuse during their early years.
- Hereditary factors: Evidence suggests a genetic component to BPD, with the disorder more common in individuals who have family members also affected by BPD.
- Neurobiological differences: Alterations in brain structure and function, particularly in areas governing emotion regulation and impulse control, are linked to BPD.
- Influences from the environment: Experiences such as neglect during childhood, early parental loss, and living in a highly dysfunctional family setting are known risk factors.
- Psychosocial elements: Complex interactions in early relationships, including issues with attachment to primary caregivers and exposure to substance abuse in the family, play a role in the onset of BPD.
- Effects of invalidating environments: Being raised in settings where one’s emotional experiences are consistently disregarded or invalidated may foster the development of BPD characteristics.
Therapeutic Approaches used to treat Borderline Personality Disorder
- Dialectical Behaviour Therapy (DBT): This therapy was specifically designed for BPD and focuses on teaching skills in mindfulness, emotional regulation, distress tolerance, and interpersonal effectiveness.
- Cognitive Behavioural Therapy (CBT): Aims to identify and challenge negative thought patterns and behaviours, helping individuals to develop healthier ways of coping with distress.
- Schema-Focused Therapy: Combines elements of CBT with other forms of therapy to help individuals identify and change complex patterns of behaviour and thought that stem from unmet needs in childhood.
- Interpersonal Psychotherapy (IPT): Tailored for BPD to enhance interpersonal skills and manage social interactions effectively, focusing on reducing interpersonal difficulties and emotional dysregulation over a 10-month comprehensive treatment period.
- Psychodynamic Psychotherapy: Aims to uncover and understand unconscious patterns and conflicts affecting behaviour and relationships, fostering insight, emotional regulation, and healthier interpersonal dynamics. Techniques include Transference-Focused Psychotherapy (TFT) and Mentalisation-Based Treatment (MBT), emphasising reflection and relationship-building.
Book Now or Learn More
Submit an intake form below or keep reading for a detailed overview of Borderline Personality Disorder.
Meet Our Therapists Who Treat BPD At Dynamic Psychotherapy
Meet the team at Dynamic Psychotherapy, who treat BPD with proven methods and personal experience. Our therapists are trained in current treatments, bringing extensive knowledge to support your mental health journey. They’re here to help you navigate through the challenges toward recovery.
Click on a therapist to view more

David Temme
David is a seasoned therapist with a strong focus on CBT Therapy. His extensive training and hands-on experience make him an expert in treating a wide range of mental health conditions, including anxiety, depression and stress management. David’s empathetic approach ensures that you feel comfortable and supported throughout your treatment journey.
Specialisations
David specialises in providing treatment for symptoms of anxiety, depression, stress management, PTSD, borderline personality and other personality disorders with CBT Therapy.
Approaches
- Eye-Movement Desensitisation and Reprocessing (EMDR)
- Schema Therapy
- Cognitive Behaviour Therapy (CBT)
- Psychodynamic Therapy
Qualifications
Accredited Mental Health Social Worker And Psychotherapist

Moulya Ramesh Kumar
Moulya Ramesh Kumar, a Melbourne-based clinical psychologist, with experience in treating Borderline Personality Disorder (BPD) along with anxiety, depression, and relationship issues for adolescents and adults. Leveraging her experience across diverse cultural backgrounds, Moulya utilises a tailored approach incorporating ISTDP, CBT, ACT, and DBT techniques. She champions a therapy grounded in empathy, authenticity, and partnership, focusing on both current challenges and deep-seated experiences for comprehensive healing.
Approaches
- Acceptance and Commitment Therapy (ACT)
- Cognitive Behavioral Therapy (CBT)
- Intensive Short-Term Dynamic Psychotherapy (ISTDP)
- Dialectical Behaviour Therapy (DBT)
- Mindfulness
Qualifications
MSc, MPhil (Clin Psych), MAPS, AMACPA

Chris Bolton
Chris Bolton is a clinical psychologist based in Melbourne, with extensive experience in treating individuals across various life stages, including adolescents, adults, and older adults. He adopts a compassionate approach, ensuring a respectful therapeutic environment where every thought and feeling is met with sensitivity and honesty. Chris has experience working with Borderline Personality Disorder (BPD), alongside managing anxiety, depression, trauma, assertiveness challenges, and issues within intimate relationships.
Approaches
- Acceptance and Commitment Therapy (ACT)
- Cognitive Behavioral Therapy (CBT)
- Intensive Short-Term Dynamic Psychotherapy (ISTDP)
- Behavioural Therapies
- Interpersonal Therapy
- Mindfulness
Qualifications
MPsych (Clinical) MAPS
Understanding and Treating Borderline Personality Disorder: A Shift from Disorder to Personality Style
Borderline Personality Disorder (BPD) is enveloped in stigma and often misunderstood, characterised by emotional turbulence and unstable relationships.
Based on a global population of approximately 7.9 billion and a prevalence rate of 1.6%, it’s estimated that around 126.4 million people worldwide are affected by BPD.2 However, when we view personality through the narrow lens of ‘disorder,’ we might overlook the broader context of an individual’s life.
The very traits that lead to a diagnosis of a personality disorder could, in another environment, be neutral or even advantageous. This suggests that what we often categorise as a disorder may sometimes be a mismatch between an individual’s inherent personality style and the specific demands or values of their current environment.
Such a perspective challenges the notion of inherent dysfunction within the person, instead pointing to the friction between their innate drives, affects, and temperament, and the external world’s expectations or lack of support.
It’s in this space of mismatch that behaviours and coping mechanisms, which are pathologised in one setting, might have been adaptive or even necessary in another.
At Dynamic Psychotherapy, we emphasise the importance of empathy and understanding in viewing BPD not just as a disorder but as a unique personality style.
Central to our discussion is the role of therapy in providing support, fostering resilience, and promoting healing. Read on as we explore the nuances of BPD and the transformative power of professional intervention, advocating for a path towards awareness, compassion, and recovery.
DSM-5 Diagnostic Criteria for BPD
Borderline Personality Disorder (BPD) is a complex psychological condition, usually diagnosed in Australia using the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5).
Symptoms are clustered to reflect a pervasive pattern of instability of interpersonal relationships, self-image and affects, and marked impulsivity beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) or the following:
- Frantic efforts to avoid real or imagined abandonment (Note: Do not include suicidal or self-mutilating behaviour covered in Criterion 5)
- A pattern of unstable and intense interpersonal relationships characterised by alternating between extremes of idealisation and devaluation
- Identity disturbance: markedly and persistently unstable self-image or sense of self
- Impulsivity in at least two areas that are potentially self-damaging (e.g. spending, sex, substance abuse, reckless driving, binge eating) (Note: Do not include suicidal or self-mutilating behaviour covered in Criterion 5)
- Recurrent suicidal behaviour, gestures, or threats, or self-mutilating behaviour
- Affective instability due to a marked reactivity of mood (e.g. intense episodic dysphoria, irritability or anxiety usually lasting a few hours and only rarely more than a few days)
- Chronic feelings of emptiness
- Inappropriate, intense anger or difficulty controlling anger (e.g. frequent displays of temper, constant anger, recurrent physical fights)
- Transient, stress-related paranoid ideation or severe dissociative symptoms
BPD can manifest in 256 different combinations of symptoms as per the DSM-5 criteria, making each person’s experience with BPD quite unique.3
Some may display more impulsive behaviours, others might struggle more with mood swings, or have difficulties in how they relate to others and view themselves.
The variety of intense symptoms can include increased prevalence of self-harm, suicidal tendencies, other co-occurring personality disorder features, issues with attachment, or difficulties in social functioning.
What Does BPD Look Like in Everyday Life?
Borderline Personality Disorder (BPD) can manifest in various ways in everyday life, affecting individuals’ thoughts, feelings, and behaviours. The symptoms and their impacts can vary widely among those with BPD, but here are some common ways it might appear in daily scenarios:
- Intense Emotional Swings: People with BPD may experience rapid mood changes over seemingly minor triggers. A day could start on a positive note, but a small perceived slight or disappointment could quickly lead to intense sadness, anger, or frustration.
- Fear of Abandonment: Everyday interactions might be overshadowed by a pervasive fear of being abandoned or left alone. Plans being cancelled or someone being late could be interpreted as evidence of abandonment or rejection, leading to desperate efforts to avoid being alone, even to the point of engaging in impulsive behaviours.
- Unstable Relationships: Relationships may be characterised by intense, unstable connections with others, swinging between idealisation (“I’ve never felt closer to anyone”) and devaluation (“They don’t care about me at all”). This can cause significant stress and confusion for both the person with BPD and their loved ones.
- Unclear or Shifting Self-Image: A person with BPD might have a continually changing idea of who they are, their values, and their desires in life. This can result in sudden changes in jobs, friends, lovers, religion, values, or goals, and may lead to feelings of emptiness and uncertainty about one’s identity.
- Impulsive, Self-Damaging Behaviours: Individuals may engage in impulsive actions like reckless driving, binge eating, substance abuse, or overspending. These behaviours often serve as a way to cope with emotional pain or distress but lead to further complications and regrets.
- Intense, Inappropriate Anger: There might be episodes of intense anger over minor issues, leading to difficulty controlling temper, arguments, physical fights, or expressing anger inappropriately. This can cause problems in personal and professional relationships.
- Chronic Feelings of Emptiness: Individuals might describe a persistent feeling of emptiness or boredom, feeling as if something is missing in their lives, which they struggle to fill with relationships, activities, or substances.
- Difficulty with Trust: Trust issues may arise, where individuals with BPD find it hard to trust others, leading to paranoia or suspicion in relationships without evident reason.
- Self-harm or Suicidal Behaviour: In response to emotional pain, misunderstanding, or fear of abandonment, individuals with BPD might engage in self-harm (cutting, burning) or experience recurring thoughts of suicidal behaviours or threats.
How Does BPD Develop?
Biological Predisposition
Research indicates that individuals possessing a genetically based sensitivity—referred to as a ‘sensitive’ genotype—are at an elevated risk of developing Borderline Personality Disorder (BPD) when exposed to certain predisposing environmental factors.
This observation is consistent with the stress-diathesis model, a concept established over three decades ago, which posits that genetic predispositions (diathesis) and environmental stressors interact to increase the likelihood of developing psychiatric conditions like BPD4
Moreover, specific genetic factors linked to BPD not only heighten the risk of concurrent disorders (comorbidity) but also predispose individuals to encountering adverse life events.
Invalidating Environment
Beyond genetic influences, empirical studies have identified a spectrum of risk factors that contribute to the onset of BPD in adolescence and adulthood.
These include a variety of childhood and parental demographic characteristics, adverse childhood experiences (ACEs), early relational difficulties, and maladaptive parenting practices.5
These findings underscore the complex interplay between genetic vulnerabilities, environmental exposures, and developmental experiences in the aetiology of BPD.
Making sense of the Research
Imagine emotions like colours; for those with BPD, the colours are incredibly vivid and intense. This intensity is not just random but can stem from a mismatch in their earliest relationships, often with their primary caregivers.
It’s not always about outright neglect or abuse; sometimes, it’s subtler, like a caregiver not responding in tune with the child’s emotional needs or missing non-verbal cues. This lack of attunement disrupts the child’s ability to learn how to manage their strong emotions.
As a result, regulating these intense feelings becomes a challenge, leading to overwhelming anxiety. To manage this anxiety, individuals with BPD might turn to what are known as defence mechanisms — think of them as emergency exits for when feelings become too much to handle.
These are psychological strategies to protect oneself from emotional stress, but they can also lead to problems. For example, impulsivity, a common trait in BPD, can be a desperate attempt to escape the suffocating grip of intense emotions, even if just for a moment.
Defence mechanisms can also manifest as alternating extremes of idealisation and devaluation in relationships — one moment, someone is seen as perfect, and the next as completely flawed.
This is because to make sense of inconsistencies in earlier relationships, the brain (a meaning making machine) categorises people and situations into all or nothing evaluations.
Therapeutic Approaches to BPD
Marsha Linehan, a clinical psychologist and the developer of Dialectical Behaviour Therapy (DBT), has publicly disclosed her own struggles with severe emotional issues similar to those experienced by individuals with Borderline Personality Disorder (BPD).
In interviews and her memoir, “Building a Life Worth Living,” Linehan has shared her personal journey, which includes hospitalisations for suicidal behaviour and struggling with severe emotional distress during her adolescence and young adulthood.
Dialectical Behaviour Therapy (DBT) treats Borderline Personality Disorder (BPD) by focusing on the development of coping skills in four key areas: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness.
- Mindfulness teaches individuals to be present in the moment, observing and accepting their thoughts and feelings without judgment. This skill helps reduce impulsivity and emotional reactivity.
- Distress Tolerance equips individuals with techniques to tolerate and survive crises without resorting to self-destructive behaviours. It emphasises accepting reality as it is, even during difficult times.
- Emotion Regulation involves learning to identify, understand, and manage intense emotions more effectively, reducing emotional vulnerability and increasing emotional resilience.
- Interpersonal Effectiveness focuses on improving relationships through assertive communication and maintaining self-respect in interactions with others.
DBT, with its comprehensive skill set, stands as a testament to the value of navigating the symptoms of BPD.
Yet, for deeper healing, an exploration into the reworking of intense emotional experiences, particularly those that trigger anxiety in relationships, is essential. This journey involves confronting and integrating the defences maintained against such experiences.
How can deeper emotional healing be achieved in those with BPD?
Difficulty in reality testing, particularly within the context of relationships, is a significant challenge for individuals with Borderline Personality Disorder (BPD).
Reality testing refers to the ability to distinguish between internal subjective experiences and external objective reality.
For individuals with BPD, intense emotions, fears of abandonment, and unstable self-image can distort perceptions of interpersonal interactions, leading to misconceptions about others’ intentions or feelings.
The Triangle of Conflict, a concept from psychodynamic therapy, particularly in approaches like Intensive Short-Term Dynamic Psychotherapy (ISTDP), provides a useful framework for understanding how difficulty in reality testing in BPD relates to underlying psychological processes.
The Triangle of Conflict consists of three components: hidden feelings, anxiety, and defence.
- Emotion refers to the primary feelings that are often not fully experienced or expressed by the individual, such as anger, sadness, or need for intimacy. In BPD, these emotions can be intense and overwhelming, challenging the individual’s capacity to experience them without extreme levels of anxiety.
- Anxiety For individuals with BPD, the anxiety triggered by mixed feelings including anger, can become intolerable, leading to impulsive actions or distorted perceptions as a way to escape or mitigate these feelings.
- Defence mechanisms are the unconscious psychological strategies used to protect oneself from the anxiety associated with these unresolved emotions. Common defences include denial, projection (attributing one’s unacceptable feelings to others), or splitting (viewing people or situations in black and white terms).
In the context of relationships, individuals with BPD may struggle with reality testing due to the interplay of intense emotions, heightened anxiety, and reliance on maladaptive defence mechanisms.
For example, the fear of abandonment (emotion) may trigger intense anxiety, leading to the use of defence mechanisms such as idealisation or devaluation of the other person.
This can distort the individual’s perception of the relationship, making it difficult to see the other person’s actions and intentions clearly.
Psychotherapy and BPD
Intensive Short-Term Dynamic Psychotherapy (ISTDP) offers a transformative perspective on Borderline Personality Disorder (BPD). Rather than framing BPD strictly as a disorder, ISTDP views it as a constellation of psychological defences that have solidified into a distinct personality style.
These defences, originally developed to protect the individual from emotional pain, may have become counterproductive, leading to the symptoms typically associated with BPD.
ISTDP aims to unravel this intricate web of defenses, offering a therapeutic pathway that enables individuals to understand and modify their emotional responses, building capacity to tolerate mixed feelings without overwhelming levels of anxiety.
By doing so, it facilitates a reshaping of the personality style into one that is more adaptive and capable of navigating the complexities of their environment.
The therapeutic work in ISTDP is not about pathologising one’s experiences but rather recognising and enhancing the individual’s innate capacity for emotional resilience and interpersonal connection.
Efficacy of ISTDP in Treating BPD and Other Personality Disorders
A study by Abbass and colleagues using ISTDP treatment with a complex population of patients, including those with BPD, provided significant insights.6
After an average of 27.7 sessions, patients treated with ISTDP exhibited significantly improved outcomes on symptom, interpersonal, and functional measures compared to controls.
Notably, treatment gains were maintained over a long-term follow-up (average of 2 years and 1 month). The ISTDP group also showed significant reductions in medication usage and increases in employment rate and work hours.
This study demonstrated more efficient treatment of a broader range of personality disorders with ISTDP compared to earlier studies, showcasing its effectiveness in treating BPD.
Conclusion
Through the therapeutic alliance and the active techniques of ISTDP, individuals develop greater emotional capacity to tolerate feelings without them triggered excessive anxiety and defenses that often cause harm to the individual, and also to their relationships.
Unhelpful defence mechanisms become redundant as the individual develops the capacity to tolerate, experience and hold feelings. They develop new, healthier ways of relating to themselves and others. This reworking of the personality structure allows for a life that is not defined by the disorder but enriched by a more nuanced and effective style of managing the emotional landscape.
In this way, ISTDP contributes to a deeper understanding and more compassionate approach to BPD, highlighting the potential for growth and change through psychotherapy.
How to Book an Appointment for help with BPD
Booking an appointment with us at Dynamic Psychotherapy for BPD support is straightforward and flexible to accommodate your needs. Here’s how you can reach out to begin your journey toward recovery:
- Phone: For direct assistance and to speak with our reception team, you can call us during business hours at 0424 220 314. They’ll help schedule your appointment at a time that suits you.
- Online Appointment Request: If you prefer online convenience, submit an appointment request through our online form here. It’s a simple process that allows you to request a session without a call.
- Email: For any inquiries or to book an appointment via email, reach out to us at [email protected]. We’ll get back to you promptly to confirm your appointment details.
Choose the method that works best for you, and let’s take the first step together towards understanding and managing BPD with care and expertise at Dynamic Psychotherapy.
FAQs About Borderline Personality Disorder
What is Borderline Personality Disorder (BPD)?
BPD is a mental health disorder characterised by unstable moods, behaviour, and relationships. It involves intense emotional experiences, difficulties in controlling emotions, and a pattern of unstable relationships.
What are the common symptoms of BPD?
Symptoms include emotional instability, feelings of worthlessness, insecurity, impulsivity, risky behaviours, fear of abandonment, and intense but unstable relationships.
What are the 4 stages of BPD?
The four stages of BPD, often referred to in the context of recovery, are:
- Emotional Vulnerability: The individual experiences intense emotional pain and feels powerless to manage it.
- Behavioural Dyscontrol: The pain leads to impulsive and harmful behaviours as a means of coping.
- Reflective Self-Understanding: The individual begins to understand their behaviour patterns and the emotions driving them.
- True Self-Reliance: The individual develops healthier coping mechanisms, leading to more stable relationships and a sense of self-identity.
Is BPD the same as bipolar disorder?
No, BPD and bipolar disorder are distinct conditions, though they can share some overlapping symptoms such as mood instability. Bipolar disorder is primarily a mood disorder with periods of depression and mania or hypomania, whereas BPD is characterized by difficulties in emotional regulation, self-image, and relationships.
What are the common triggers for borderline personality disorder?
Triggers for someone with BPD can vary widely but often involve situations that evoke intense emotional responses. Common triggers include fear of abandonment or rejection, interpersonal conflicts, feelings of failure or inadequacy, and reminders of traumatic events.
What age does BPD peak?
Symptoms of Borderline Personality Disorder typically peak in late adolescence or early adulthood, often around the age of late teens to early 20s.
While symptoms can persist over time, many individuals experience a decrease in the severity and frequency of symptoms as they get older, particularly with appropriate treatment.
Studies suggest that with proper therapy and support, many people with BPD can achieve significant improvement in their symptoms and overall functioning.
Have any questions, or ready to book an Appointment?
Our friendly Reception team is here to help you.
Footnotes
- ↩︎
- Chapman, J., Jamil, R. T., & Fleisher, C. (2017). Borderline personality disorder. ↩︎
- Keefe, J. R., Kim, T. T., DeRubeis, R. J., Streiner, D. L., Links, P. S., & McMain, S. F. (2021). Treatment selection in borderline personality disorder between dialectical behavior therapy and psychodynamic psychiatric management. Psychological Medicine, 51(11), 1829-1837. ↩︎
- Stone, M. H. (1980). The borderline syndromes: Constitution, personality, and adaptation. (No Title). ↩︎
- Chanen, A. M., & Kaess, M. (2012). Developmental pathways to borderline personality disorder. Current psychiatry reports, 14(1), 45-53. ↩︎
- Abbass, A., Town, J., & Driessen, E. (2012). Intensive short-term dynamic psychotherapy: a systematic review and meta-analysis of outcome research. Harvard review of psychiatry, 20(2), 97-108. ↩︎